302views
Almost 10 years ago, Goldman Sachs published a report, in which it predicted Chinese GDP to overtake the USA’s GDP by 2020. Today, this prognosis looks like a far-fetched dream as China has recently been riding a wild economic horse. When Chinese economy was growing, its demand for various products and services contributed to the economic growth of emerging markets across the world. The deteriorating performance of Chinese economy over the past few years appears to have started adversely affecting these markets. Will the emerging markets be able to successfully sustain in future?
China witnessed a spectacular and continued rise of its GDP during major part of last three decades. However, end of 2007 saw a turning point, and the country’s economic growth rate cooled off from 14.2% still in 2007 down to 9.6% in 2008, reaching mere 7.4% in the first quarter of 2014. This single digit growth would be more than satisfactory for a lot of economies. However, for China, which regularly recorded double digit rates, this extended period of slower growth is disappointing, with some calling it as ‘an end of an era’.
For years, China was enjoying relentless economic growth through massive investments, exemplary rise in exports, as well as abundance of labor force which was available at low wages. Due to these factors, economists started referring to China’s economic growth model as an investment-and-export driven model. This model has played a key role in driving exports also from emerging markets such as Latin America, Asia, and Middle East, as there was substantial demand for commodities from China’s end to support its domestic consumption as well as export requirements. With the weakening of foreign demand and internal consumption, China’s export demands have considerably weakened, leading to declining prices of export-related commodities and resulting in an adverse impact on emerging markets’ GDPs.
Is the Slowdown for Real?
China’s economic slowdown has not only been reflected in its modest GDP growth figures, but also in several other negative trends that have been observed. These include a continuous decline in the percentage of fixed-asset investments as a part of China’s GDP. Investments contracted from 24.8% in 2007 to 19.6% in 2013. Reduction of fixed-asset investments is likely to negatively contribute towards a country’s economic slowdown by adversely affecting sectors such as real estate, infrastructure, machinery, metals, and construction.
Moreover, yuan has depreciated against US dollar (with average exchange rate of 7.9 in 2006 down to 6.26 in April 2014). In addition to this, Purchasing Managers’ Index (PMI), which is a composite index of sub-indicators (production level, new orders, supplier deliveries, inventories, and employment level), has plunged from 52.9 in 2006 to 48.3 in April 2014, below the middle value (50), thus indicating some contraction of China’s manufacturing industry. This industry contributes significantly to China’s GDP, therefore, the industry’s deterioration has a direct adverse effect on China’s economy.
This negative twist in China’s economic growth story is believed to be a result of a synergetic effect of various internal and external factors, some of which include:
-
Over-reliance on abundant supply of low-cost labor. For decades, China has based its growth on production of goods requiring high amount of cheap manual labor. However, as the economy continued growing, the demand for higher wages has increased, pumping up the labor cost. This cost is contributing to the inflation of products’ export prices, which is ultimately translating to a lower demand of Chinese goods.
-
The focus of Chinese workforce has been shifting from rural agriculture to urban manufacturing. The government has been taking steps to propel this transition in order to boost economic growth, prosperity, and industrialization. As more and more Chinese moved to urban areas, gradually, the transition has started yielding diminishing returns mainly due to saturation in the manufacturing industry.
-
Europe has also played a villainous role in China’s story. It has been one of China’s largest export markets but has recently been extending a significantly low demand for commodities and products from China. In 2007, the European Union accounted for 20.1% of all the exports from China. This percentage has fallen to 16.3% in 2012.
Chinese Leaders React
The Chinese government is in a reactive mode and has been unveiling a plethora of actions to bolster growth. The overall approach looks conservative in nature with a targeted GDP growth of 7.5% for this year, after recording a growth of 7.7% in 2013.
In an attempt to improve the situation, some of the expected financial and fiscal reforms are in the pipeline. Liberalizing bank deposit rates and relaxing entry barriers for private investment are some of the moves to be implemented by 2020. Various property measures (such as relaxing home purchase rules, providing tax subsidies, or cutting down payments) are planned to be introduced (based on local demands and conditions prevailing in a particular city) in order to balance the property market as a whole. A target of creating 10 million new jobs in Beijing has also been set for 2014. The underlying motive of all the rescue measures is strengthening the Chinese economy’s reliance on domestic consumption and services.
Influence on Emerging Markets
Undoubtedly, swing of the Chinese economy towards consumption and services is expected to considerably affect all the connected economies, several of them being emerging markets economies (EMEs). Commodity producing emerging markets such as Latin America, Middle East, parts of Africa and Asia are likely to be affected. Within this group, metal producers will probably suffer the most, as China had a significant demand for iron ore, steel, and copper during its investment boom phase. Within this subgroup, economies which are running current account deficits are forecast to be more susceptible to the ill-effects of China’s economic slowdown.
As China tilts towards domestic consumption, Latin America has started to witness a dawdling growth as the region’s growth rate dropped from an average of 4.3% in the period of 2004-2011 to 2.6% currently. For instance, as Chile depends heavily on copper exports to sustain its economic expansion, the country has been regularly reporting sluggish growth rates (5.8%, 5.9%, and 5.6% in 2010, 2011, and 2012, respectively) due to the decline in the price of copper, largely fueled by a lower demand from China. In addition to this, Brazil and Mexico are struggling to survive through falling benchmark stock indexes. The fall is mainly due to declining prices of commodities, as exports to China from Brazil and Mexico have weakened.
Middle East will probably register both positive and negative effects of China’s economic slowdown. One of the ill-effects could be reduction in oil prices, from US$140 per barrel in 2008 to approximately US$80 per barrel by the end of 2014, due to China’s lower demand of oil. On the positive side, Middle East is strengthening its position as an attractive region with long-term growth since China is being considered as a slightly less attractive option for investment by a majority of investors. This is mainly due to Middle East’s good infrastructure and accelerated development of industries such as defense, chemical, and automotive, and not only traditionally developed energy and petrochemicals.
The impact on African countries is expected to be negative primarily due to declining commodity prices. As Africa’s growth substantially depends on its exports to China, some African commodity exporters, such as Zambia, Sudan, and Angola, have started to feel the strain as China’s demand for commodities is weakening. This weakened demand has led to lower prices of commodities such as aluminum, copper, and oil, which registered a y-o-y decline by 4%, 9.5%, and 5.4%, respectively in January 2013. Zambia is likely to receive the strongest hit as copper constitutes almost 80% of the country’s total exports and reduction in copper prices could make its current account deficit to account for almost 4% of GDP in 2014.
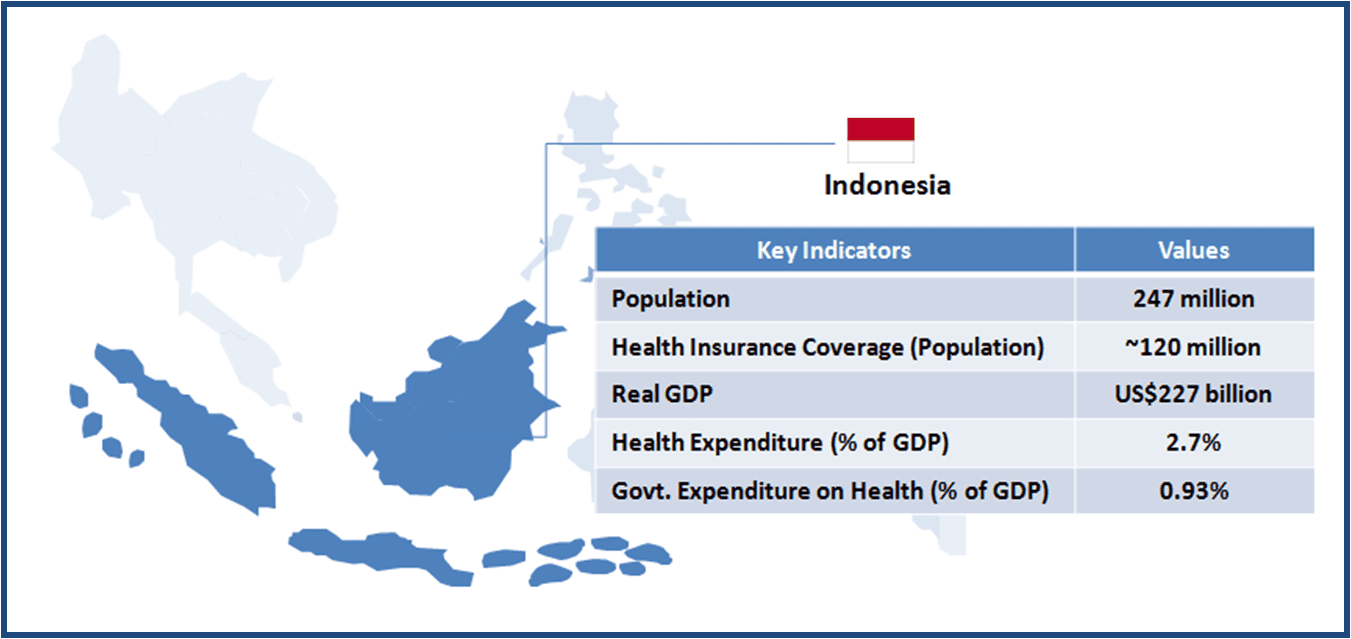
Effect of China’s economic slowdown will vary from country to country in case of Asia. Countries such as Indonesia and Philippines, which have significant domestic demand, would be less adversely affected as they are less dependent on commodities exports to China. China’s unstable economy has spurred new investments in other growing Asian economies such as Cambodia. India is also likely to benefit from the ability to import oil at lower prices, which are pushed down by China’s weakened demand for oil. At the same time, however, export of cotton and metals such as copper and iron ore from India to China is dampened, adversely affecting India’s economy.
While EMEs have already been witnessing a lower demand from their traditional trading partners such as European Union and the USA, China’s slowdown will be an added burden to their economies.

It’s Touch and Go
It is rather evident that Chinese economic slowdown is having an adverse impact on emerging countries across Africa, Asia, and Latin America. One can hope that the measures taken by the Chinese leadership to curtail the slowdown will soon start taking effect and gradually lift up the economy, and in doing so, control the extent of damage spilling over many emerging countries and their economies.
In the event that the Chinese economy is unable to recover from this period of slowdown soon, it will continue to be a terrible blow to the economic ambitions of several emerging markets, especially those in Africa and parts of Asia-Pacific, which are heavily reliant on Chinese investment and trade relations.
Simultaneously to absorbing fewer production inputs imported from emerging countries, it is worth noting that China’s role in world economics might start to alter as it transforms to a consumption-led economy. This transformation is likely to slowly increase China’s appetite for imports of products and services, apart from traditional commodities-focused imports. It will be interesting to observe whether and how some of the emerging economies will attempt to satisfy this new Chinese hunger for goods extending beyond simple commodities.







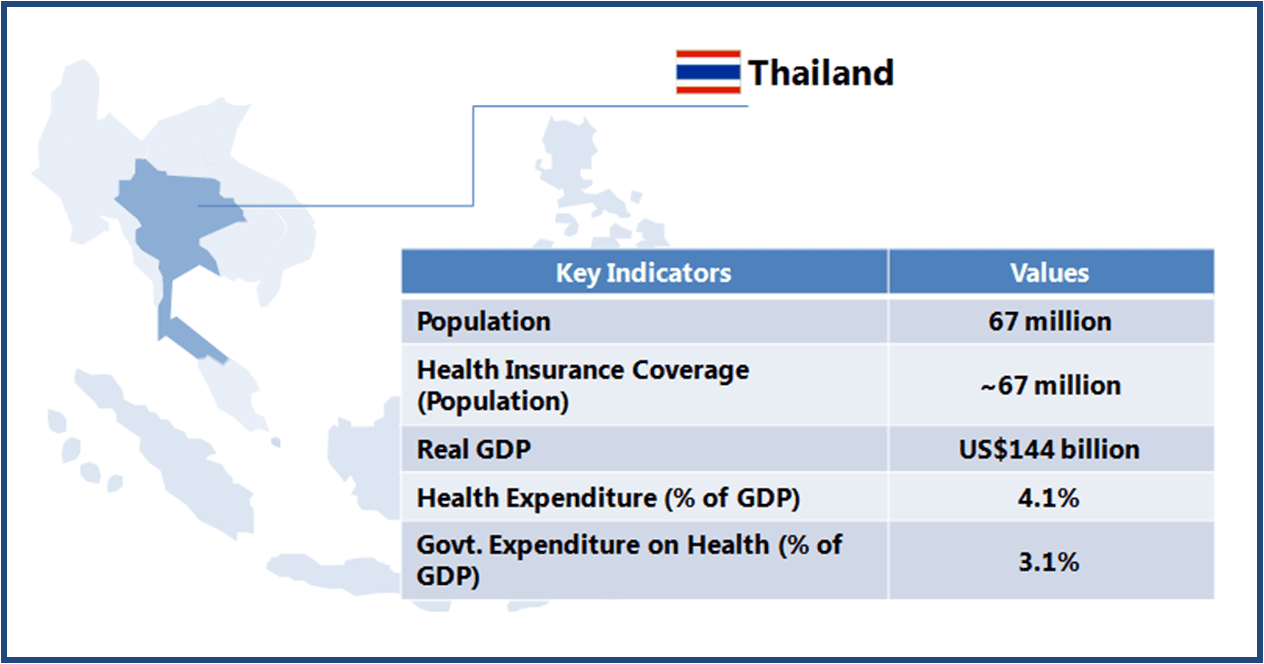 Thailand boasts of world class medical facilities (especially in the private healthcare sector), and is among the world’s largest medical tourism markets. The government is looking to further develop Thailand into an “International Health Center for Excellence” under its second strategic five-year plan (2012-2016).
Thailand boasts of world class medical facilities (especially in the private healthcare sector), and is among the world’s largest medical tourism markets. The government is looking to further develop Thailand into an “International Health Center for Excellence” under its second strategic five-year plan (2012-2016).